EMF Cancer Promotion: An Old Idea Makes a Strong Comeback
Large Study Shows Recent, But Not Lifetime, Exposures Lead to Brain Tumors
Power-frequency magnetic fields can promote brain tumors, according to the largest epidemiological study of its kind ever undertaken. The study promises to breathe new life into the idea that extremely low frequency (ELF) EMFs are more likely to be cancer promoters than causes of cancer. This hypothesis gained support a generation ago but has lost currency in recent years.
The new results, published online earlier this month by the journal Cancer Epidemiology, Biomarkers & Prevention, come from INTEROCC, an international project with seven participating countries designed to investigate occupational health risks from chemicals and EMFs.1 The project is directed by Elisabeth Cardis at CREAL in Barcelona with $1.5 million from the U.S. National Institutes of Health (though none of the tumor cases are from the U.S.).
The INTEROCC team found that those who were exposed to elevated EMF exposures at work during the five years prior to diagnosis had significantly higher rates of glioma compared to those who were least exposed during that time on the job.2 The greater the exposure, the greater the tumor risk. Those who were most highly exposed had approximately 67% more tumors. (The controls were the lowest-exposed workers from the same study population.) The risks for meningioma, a mostly benign type of brain tumor, were smaller than for glioma.
The key concept here is cancer promotion, as opposed to cancer causation or initiation. According to the prevailing paradigm, cancer develops as a two- or three-step process. First, a cell is transformed into a cancer cell; this is initiation. The cells grow into a tumor with the help of a promoter, which helps them evade the body’s immune system. (The third stage is progression, but we won’t get into that here.)
The INTEROCC results point to EMFs as a promoter, and not as an initiator. The EMFs do not cause cancer, rather they foster its growth and development. The new finding will help sidestep the most often cited objection to the idea that magnetic fields are linked to cancer because no EMF–induced DNA breaks would be required.
As shown in the first panel of the triptych below (Figure 1a in the INTEROCC paper), the risk of developing a glioma increases with higher magnetic field exposures within five years of diagnosis.2 The trend is highly significant, with p<0.0001; that is, there is less than one chance in 10,000 that this is a random outcome. No similar increases were seen for longer exposure times, 5-9 years or 10 years or more (the second and third panels).
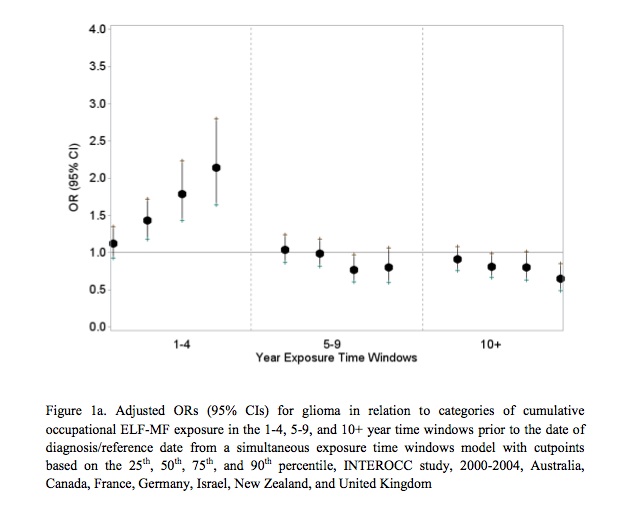 The intensity of the magnetic field increases as one moves along the x-axis within each time window.
The intensity of the magnetic field increases as one moves along the x-axis within each time window.
(Note: Exposures within a year of diagnosis were excluded.2)
If the cases from all three panels are combined, that is, one ignores when the workers were exposed —early or late in their careers— and look only at total exposure to magnetic fields, the promotional effect disappears. INTEROCC sees no association between brain tumors and cumulative EMF lifetime exposures.
“The suggestion that EMFs are working at the later stages of carcinogenesis is very interesting and potentially spot on,” Tony Miller, a professor emeritus at the University of Toronto, told Microwave News. Miller helped lead a Canadian-French utility worker study in the 1990s (see below).
A Short History of Occupational Brain Tumor Studies
The idea that EMFs may promote cancer is by no means new. In fact, promotion was the suggested mechanism in the first report of an association with brain tumors by Ruey Lin thirty years ago. At the time Lin, who was with the Maryland health department, told Microwave News that his work “supports the theory that non-ionizing radiation may be a brain tumor promoting agent” (see MWN, Oct84, p.2). He reiterated this view in his paper, when it was published the following year. (Lin later went home to Taiwan where in 2012 he was an unsuccessful candidate for the country’s vice presidency.)
By 1990, at least a dozen EMF studies, many of them occupational, pointed to an association. “I definitely feel the case has always been the most consistent for brain tumors,” Nancy Wertheimer told us back then (see MWN, M/A90, p.1). A similar assessment was offered not long afterwards by an advisory panel assembled by the U.K. National Radiological Protection Board (NRPB), chaired by Sir Richard Doll.3
Even so, assessing EMF exposure was still very primitive: Most studies used job titles as surrogates, which were imprecise. By the 1990s, measured fields were coming into play, but this raised another thorny issue: How best to estimate a worker’s past exposure —possibly reaching back over a lifetime— when all that was available was a single spot measurement or a 24-hour average. These second generation studies were also hampered by having a small number of subjects.
Birgitta Floderus in Sweden was the first to test the promotion hypothesis using measured fields. She focused on the job held the longest during the ten years prior to diagnosis and she too saw an association, but with only a weak dose-response (see MWN, S/O92, p.1). Her case-control study, with 261 brain tumor cases, was published in 1993.
Over the next couple of years, two studies of electrical workers appeared: one from Canada and France and one from the U.S., each with about 150-160 brain tumor cases. They offered somewhat different results. The Canadian-French study pointed to a leukemia risk, and though the risk of developing a brain tumor was elevated, it did not reach statistical significance (see MWN, M/A94 p.1). In a cohort study of U.S. workers, David Savitz and Dana Loomis found an excess of brain cancer but not leukemia. Like Floderus, they looked at a ten-year window before diagnosis. Without specifically mentioning the promotion hypothesis, Savitz and Loomis reported that the risk for the same amount of exposure “was markedly greater” in that time window, “suggesting a relatively short latency period.”
Further support for promotion came in 2002 when Paul Villeneuve published the results of what was then the largest study ever done, with 543 brain tumor cases (open access paper).4 Villeneuve took a different tack from Floderus and Savitz-Loomis: Rather than looking at a specific window of exposure, Villeneuve compared the risks for those with the highest magnetic field exposures in their most recent jobs to those with the highest exposures in their first jobs. The latter group had a risk that was close to five times that of the controls, though it was not significant. For those with the recent high exposures the risk was more than double that of the first job group: It soared to 12.5-times that of controls, a significant increase.
What Villeneuve saw is consistent with promotion, he told us recently. The results should be interpreted with “caution” because of the small number of cases with high exposures, he warned in his 2002 paper. Today, Villeneuve is at Carleton University.
Size Matters, As Does Detailed Exposure Assessment
Now comes INTEROCC, a case-control study with 3,761 brain tumor cases (1,939 glioma and 1,822 meningioma), more than all the previous efforts combined and about seven times bigger than Villeneuve’s. “INTEROCC is different from past studies,” says Joe Bowman, an industrial hygienist at NIOSH in Cincinnati, who was responsible for assessing EMF exposures for the project.5 “It is far larger than other occupational case-control studies.”
Not only is INTEROCC the biggest study of its kind, it also features the most thorough exposure assessment ever attempted. It uses what is known as a job-exposure matrix (JEM) to link job titles to estimates of magnetic field exposure. Bowman originally devised the JEM in the mid-2000’s. The enhanced JEM used by INTEROCC, based on personal measurements made in eight different countries, features 409 different job categories.6 One type of exposure was not included in Bowman’s JEM, however, that from GSM phones (see “What About Cell Phones?”).
A lot of the data used in INTEROCC was actually collected by the INTERPHONE project (see “Freaky or What?”) and later analyses will take into account INTERPHONE interviews on job histories and occupational EMF exposures. “We are now working on an even more detailed assessment, which will include both ELF and RF exposures,” Bowman said.
INTEROCC’s large number of subjects and the comprehensive exposure assessment presents a more detailed picture of the brain tumor risks. For the first time a dose-response analysis could be done for exposures within different exposure windows (Figure 1a above). Without those time windows, the INTEROCC analysis does not point to a promotion effect, or any EMF–brain tumor link at all.
The importance of those time windows can be seen in a case-control study published five years ago by a group at the Radiation Epidemiology Branch of the U.S. National Cancer Institute (NCI), led by Martha Linet and Peter Inskip (Joe Coble is the first author). The study was relatively large, with 686 brain tumor cases, including 489 glioma. Though still much smaller than INTEROCC, the NCI study comes in as the second largest study ever, bigger than Villeneuve’s. The exposure assessment was similar to INTEROCC’s; in fact, the NCI used the earlier version of Bowman’s JEM. (Bowman is a coauthor of the NCI paper.) Linet and Inskip report seeing no association, even though they had used what they called “a novel exposure assessment method.” What NCI did not do is test for promotion using time windows.
If windowing had not been applied to the INTEROCC analysis, the NCI and INTEROCC studies would have yielded “consistent results,” Bowman told Microwave News.
How Long a Time Window?
How long does it take EMFs to promote cancer cells into a brain tumor big enough to be diagnosed? The short answer is no one knows. This means the best anyone can do is to take an educated guess. INTEROCC picked a five-year window for tumor promotion, which others have used in the past. But it could have been shorter or longer.
Michelle Turner, the lead author of the new INTEROCC paper, explained that the five-year window was the team’s a priori hypothesis. “No other cut-points were used in the analysis,” she told us from Barcelona.
Previously, Birgitta Floderus in Sweden and Savitz & Loomis in the U.S. used a ten-year window. This longer time period may well have been selected to collect enough cases in order to allow them to test the promotion hypothesis. A 2001 cohort study from the U.K.’s University of Birmingham by Malcolm Harrington and Tom Sorahan used a five-year window, like INTEROCC, and ended up with only 38 cases with any exposure to magnetic fields during that time period.7 In comparison, the Savitz-Loomis study had three times as many (113) with some exposure during their ten-year window, with 43 in the most exposed group, compared to only two highly exposed cases in the 2001 Birmingham study.
Like the Birmingham group, the Danish Cancer Society has published the results of its own cohort studies, which also did not see an association between magnetic fields and brain tumors.8,9,10 (Yes, there is a Danish cohort study on EMFs, as well as on cell phones; see “Freaky or What?”).
David Savitz in 2001: Time to “Share the Good News”
In 1995, when the Savitz-Loomis study was published, Savitz didn’t mince words about what they had found: “Our study adds evidence that is clearly positive for brain cancer,” he told EPRI, the research arm of the electric utility industry.11 Yet, a few years later, in an editorial accompanying the Birmingham cohort paper in Occupational and Environmental Medicine, Savitz recounted that, with the benefits of an EPRI–sponsored analysis designed to “explain and reconcile discrepant findings that had been published over the previous decade,” he had reached the conclusion that, for brain cancer, “a fairly complete answer” was in hand.12 There was no risk and no real point of doing any further research, according to Savitz.13 Here’s part of what he wrote:
“We may well be doing a disservice not to share the good news more energetically and widely —electric utility workers and other similar such workers do seem not be at measurably increased risk of brain cancer.”
Villeneuve’s study came out the following year, but by that time, research money had dried up and no one paid much attention. Indeed, nothing much happened for the next ten years except for the NCI study which, as we have seen, endorsed the prevailing view that EMFs don’t entail a brain tumor risk.
Whether INTEROCC will reopen the door that Savitz helped slam shut remains to be seen. Meanwhile, Cardis’s project team is moving forward to look at occupational exposures to both ELF and RF, based on the INTERPHONE interviews, as well as the the possible influence of chemical exposures. (So far, no cancer risks attributable to chemicals have been reported.)14 “A manuscript examining interactions between occupational chemical and ELF exposure is currently in preparation,” Turner said.
June 9, 2017
A new paper from the INTEROCC project shows “no clear evidence for interactions between occupational ELF and chemical exposures in relation to glioma or meningioma risk.” It appears in Occupational & Environmental Medicine, and was posted today.
__________________
1. The seven countries are Australia, Canada, France, Germany, Israel, New Zealand and the U.K. When the project was first announced in 2007, France and Italy were among the participants. See our report, Interphone 2.0 from 2007.
2. The INTEROCC team used five-year windows, but did not count exposures in the first year on the job prior to diagnosis. As Elisabeth Cardis explained to us, this was in order to “exclude exposures which might have occurred after a tumor started but before its diagnosis.”
3. This appraisal appears in “Electromagnetic Fields and the Risk of Cancer, Report of an Advisory Group on Non-Ionising Radiation,” Documents of the NRPB, Vol.3, No.1, 1992, p.130.
4. Paul Villeneuve found that those exposed to the highest magnetic fields were likely to develop the most aggressive types of brain tumors (grade III or IV astrocytoma, also known as glioblastoma multiforme). Based on this finding, he concluded that his results were “consistent with the hypothesis that magnetic fields act at the promotional stage.” INTEROCC investigated whether the risks were different for high- and low-grade glioma, but did not find any differences (see the INTEROCC paper’s Supplementary Table S4).
5. While Joe Bowman was responsible for the assessment of EMF exposures, Martie van Tongeren of the Institute of Occupational Medicine in Scotland was in charge of INTEROCC’s exposure assessment for chemicals. For details, see her open access paper. van Tongeren was also a coauthor of the 1997 and 2001 Birmingham papers.
6. The original JEM, described by Bowman in a 2007 paper, had 250 job categories. For details on the differences between the 2007 and the new JEM, see the ELFJEM page on the CREAL Web site.
7. Tom Sorahan published an update of the Birmingham study earlier this year. This time, he had many more cases (372), though still far fewer than INTEROCC. Expanding the time window from five to ten years also helped increase the number of cases in that promotion window to 148. He did not see a promotion effect. Sorahan is also a coauthor, with Malcolm Harrington, of an earlier paper published in 1997 (open access); this study included a total of 112 cases of brain cancer.
8. While preparing this article, we noted a trend, which, with some exceptions, shows that case-control studies tend to show an association between EMFs and brain tumors, while cohort studies do not. We asked Paul Villeneuve which of the two would be more likely to reveal an association, if one did exist. This is what he told us: “Cohort studies, in my view, are always preferred wherever possible. They avoid issues related to participation bias, and in some cases recall. However, for brain cancer outcomes due to their rarity cohorts are fairly impractical.” We posed the same question to Tom Sorahan. He replied: “The INTEROCC study is based on a larger number of cases which is a strength but has the disadvantages of relying on volunteers participating with the researchers, only having self-reported work histories and lacking real knowledge about the exposures in many different workplaces. So in general, the cohort study of specific workplaces is to be preferred. Having said that I did not consider exposures in the most recent five years in my 2014 paper.”
9. The original Danish cohort study of brain tumors among electric utility workers was published in 1998 (open access paper). An update followed in 2007. Christoffer Johansen of the Danish Cancer Society was the lead author of both papers. Joachim Schüz, now with IARC, was a coauthor of the 2007 update. Schüz is also a coauthor of the new INTEROCC paper.
10. In 1993, two years before the Savitz-Loomis paper came out, Jack Sahl published a mixed case-control and cohort study which showed no EMF–brain tumor association. The number of cases in the case-control part was very small: just 32 cases.
11. EPRI Journal, March/April 1995, p.17.
12. The electric utility industry pushed the view that, because the Canadian-French study saw a stronger link to leukemia than to brain cancer and the Savitz-Loomis study pointed to a stronger link to brain cancer than leukemia, they were inconsistent. As Stan Sussman, then the manager of EPRI's EMF program, stated at the time, “The inconsistencies in results among studies underscore our limited understanding of the risks of exposure to EMF among utility workers…” (EPRI Journal, March/April 1995, p.17).
13. It might be pointed out that, for most of the 1990s, David Savitz was an EPRI contractor. EPRI, the research arm of the electric utility industry, sponsored his and Dana Loomis’s epidemiological study of electric utility workers at a cost of some $5 million, about $10 million in today’s dollars.
14. The negative findings on chemical risks are reported in these two papers.